
The United States Department of Labor reported over one million injuries and illnesses requiring days away from work among private industry, state, and local government employees. Of these injuries and illnesses, 16.6% were low back-related, resulting in 191,479 low back injuries requiring eight days away from work. Low back pain (LBP) is classified into three categories: nonspecific LBP, potentially associated with radiculopathy or spinal stenosis, and potentially associated with another specific spinal cause. Lumbar intervertebral disc (IVD) herniation is one of the most common spinal degenerative disorders, leading to LBP associated with radiculopathy.
To better understand the role of IVD in the development or persistence of LBP and spinal stenosis, many systematic studies have focused on lumbar spinal height changes associated with various positions and movements. Natural IVD height preservation is so important that the biomedical field has examined the use of growth factors for IVD biologic regeneration.
People spend about 61% of their time standing in the work and home environment. Although prolonged weight-bearing postures, such as standing and walking, have been associated with decreased spine height, some studies have reported that seated weight-bearing postures could result in spine height gain. Sustained and repetitive lumbar extension postures frequently occur after periods of prolonged unloading, such as sleep. People presenting with direct preferences that include lumbar extension tend to respond well to exercises geared toward trunk extension.
Standing back extension exercises have been reported to prevent back pain episodes and decrease back pain in care workers. Standing exercises have the advantage of being functional and can be easily performed in both work and home settings. Lumbar extension range of motion (ROM) positively correlates with symptoms’ centralization in LBP patients. Clinicians assess symptoms’ centralization, which refers to symptoms retreating towards the spine midline in response to repeated movements or guided positioning.
Previous studies investigated the effects of postures and movements in lying (unloaded) or seated positions on spinal height. Most rehabilitation programs focused on LBP prevention and management use both repetitive and/or sustained spinal extension exercises to improve patients’ outcomes. However, no study to date has investigated the effects of standing extension postures on spinal height, pain, centralization, and function. The point of this study is to find out what happens to spinal height, pain, symptom centralization, and functional measures when the trunk is extended while standing, both continuously and over and over again. (Harrison et al.)
A study aimed to evaluate the effects of standing sustained trunk extension (STE) and repetitive trunk extension (RTE) on spinal height, pain, centralization, and function after a period of spinal loading. A pre-test, post-test comparison group design was used, with a mixed design comparing the type of trunk extension and time between subjects.
A study was conducted on 35 subjects with musculoskeletal low back pain (LBP) from physician offices, sports medicine clinics, and the Fredericksburg community. The study included subjects with LBP and a preference for trunk extension, regardless of chronic symptoms. The inclusion criteria included the ability to come twice to the physical therapy clinic, age 18–80, the ability to stand and sit for 5 minutes, and low back pain on the Numerical Pain Rating Scale (NPRS) of at least 2/10. Exclusion criteria included pregnancy, history of back surgery or spinal fractures, current history of acute systemic infection, active inflammatory disease, or malignancy, and those involved in legal or compensation claims for their back symptoms.
The study aimed to investigate the effects of standing RTE and standing STE on spinal growth and pain in low-back pain patients. Participants attended two physical therapy sessions, with each participant watching an audio-visual PowerPoint presentation explaining the study, test procedures, and including a video describing the interventions. Written informed consent was obtained, and directional preference was determined using guidelines set forth in the directional preference definition and based on standards set forth in randomized clinical trials.
For session 1., a questionnaire including pertinent medical history was completed, and participants completed a Numerical Pain Rating Scale (NPRS) to rate their current, minimum, maximum, and average LBP over the last two days. They also completed a Body Diagram for indicating the location of symptoms, a Modified Oswestry LBP questionnaire, and a Fear Avoidance Belief Questionnaire. A researcher recorded the participant’s height and weight.
At the beginning of data collection, a randomization plan generator assigned each participant to one of two interventions: standing RTE at a rate of 10 per 45 seconds, repeated five times with 15-second rest breaks; or standing STE for 5 x 45 seconds with 15-second rest breaks. Each participant completed one intervention. The test sequence after a 10-minute period of trunk unloading in a supine posture to ensure spinal height was normalized was used to measure spinal height.
Participants repositioned on the stadiometer and measured their spinal height after a relaxed exhalation, a five-minute period of loaded upright sitting with a 4.5 kg bag secured on each shoulder, and an additional five minutes of sitting without load. The participant then underwent one intervention for 5 minutes, as previously described, according to the randomization assignment.
Participants received home instructions, and during the follow-up two-week period, they continued to take their medications as their primary healthcare provider had instructed them to do. A sheet including home exercise instructions was provided to each participant, and they completed a sheet recording home exercise compliance.
For session 2, participants completed the same questionnaires, trunk unloading procedure, and four stadiometric measurements as in session 1. They scored their low back and lower extremity symptoms using NPRS and mapped their pain on a body pain diagram. The principal investigator was involved with data collection, supervised positioning in the stadiometer, and stadiometric measurements.
Data analysis was carried out using Excel and SPSS 23.0 for Windows. Descriptive statistics, including mean, median, mode, standard deviation, minimum and maximum values, and frequency counts, were collected for age, height, weight, body mass index, pain, centralization, function (Modified Oswestry LBP Disability Questionnaire), FABQ, spinal height, and spinal height changes after repetitive and sustained standing trunk extension after a period of spinal loading. Independent t-tests and Mann-Whitney Whitney-U were used to assess differences between the groups for these variables at the beginning of data collection. Levene’s test and the Shapiro-Wilk test of normality were used to test for variance and measurements of the distribution of spinal height, changes in spinal height, degrees of spinal extension, pain, and function outcomes. A Wilcoxon sign-rank test was used to assess differences in spinal height, centralization, and pain outcomes following STE and RTE postures.
The study examined differences in spinal height change and function outcomes due to sustained and repetitive standing trunk extension after spinal loading. Mixed ANOVAs and post-hoc paired t-tests were conducted to explore significant differences. Kruskal-Wallis examined pain levels and current pain as a result of STE and RTE after spinal loading. Alpha level was set at 0.05 for significance.
A study involving 35 participants was conducted to evaluate the effectiveness of a home exercise program for reducing pain. The participants were divided into two groups: the RTE group (men and women) and the STE group (six men and nine women). The study found that both groups reported pain reduction before the second session, but the STE group showed a larger reduction in pain. The Modified Oswestry showed improvement in both groups, but neither achieved a 6-point minimal clinically important difference (MCID). Both groups were centralized by a median of 1, with no difference between the groups. The study found that the STE group showed a larger reduction in most pain compared to the RTE group, and the STE group showed a smaller reduction in current pain compared to the RTE group.
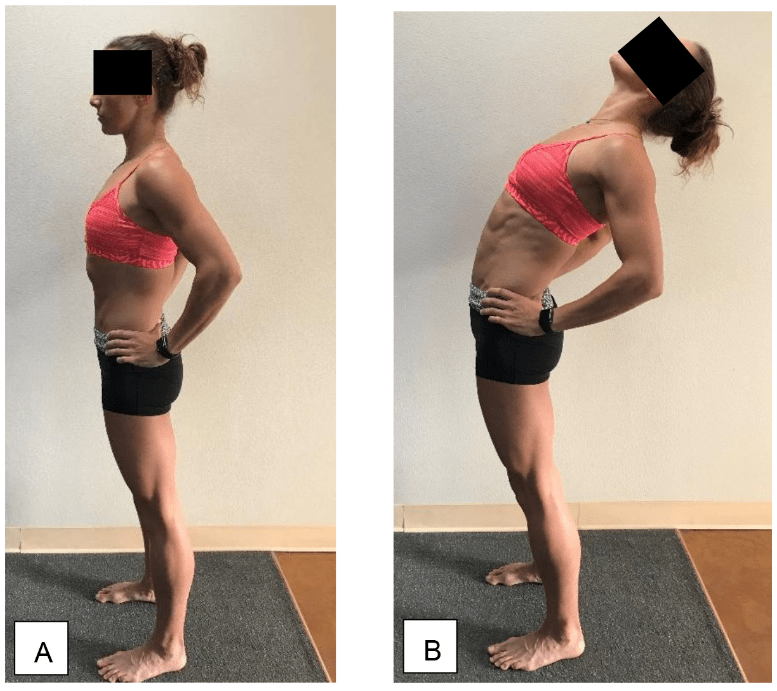
This study evaluates spine growth during standing extension postures commonly used in Mechanical Diagnosis and Therapy (the McKenzie Method) in a population of people with low back pain (LBP). The study was designed to avoid exclusion based on age and lumbar pathology, as it aimed to better understand the effect of standing trunk extension postures on these populations. Standing trunk extension may be a safer option for cardiovascular patients due to less hemodynamic demand compared to prone or supine lying trunk extension. It can also be more practical and easier to achieve for subjects depending on convenience and physical ability.
The results indicate that standing trunk extension posture for 45 seconds repeated five times caused greater spine growth compared to RTE posture for 10 repetitions repeated five times within five minutes, showing large effect sizes. LBP decreased to a greater extent when participants sustained versus repetitive trunk extension in standing. It is possible that the RTE group showed less spinal height increase and pain reduction due to their higher average age and chronicity of symptoms. These findings suggest that people who respond favourably to standing trunk extension exercise could use such postures and movements to alleviate their LBP and improve spine height while in a weight-bearing position.
People with low back pain (LBP) showed significant improvements in spine growth and pain relief during standing STE compared to RTE. These findings suggest that these postures and movements can alleviate LBP and improve spine height while in a weight-bearing position. Sustained trunk extension may be more effective in restoring spinal height loss than RTE intervention and offers an alternative ergonomic postural option for rehydrating lumbar IVDs.
At Dynamic Disc Designs, we create dynamic spinal models to help clinicians explain sources as well as proposed solutions for low back and neck pain.